Adult scoliosis is the intersection of spinal deformity and the degenerating spine.
 In de-novo degenerative spinal deformity patients often present with loss of lumbar lordosis and mild to moderate sagittal plane imbalance. Coronal plane deformity is typically mild. However, progressive back pain from the degeneration or buttock and leg pains from lumbar spinal stenosis (nerve pinching from bone spurs) may drive a patient to seek treatment.
In de-novo degenerative spinal deformity patients often present with loss of lumbar lordosis and mild to moderate sagittal plane imbalance. Coronal plane deformity is typically mild. However, progressive back pain from the degeneration or buttock and leg pains from lumbar spinal stenosis (nerve pinching from bone spurs) may drive a patient to seek treatment.
Patients with pre-existing adolescent idiopathic scoliosis may degenerate either the scoliosis or the spine around the scoliosis because of the normal spinal compressive forces being transmitted through tipped or curved vertebrae and discs. Patients may present with coronal (shifted) or sagittal plane (stooped) deformity. Patients who have developed significant lumbar spinal stenosis (bone spurs pinching nerves) may demonstrate neurologic deficits related to nerve root compression. Or a collapsing spine syndrome may be present with progressive pain and spinal imbalance.
Again, non-operative treatments in adult patients are primary, with osteoporosis treatment, physical therapy and if necessary, injections. If these fail, and either the scoliosis or the disability associated with it progresses, surgery may be necessary.
Lordosis
Lordosis is a condition consisting of an excessive inward curve of the spine causes the body to improperly distribute mechanical stress from movement such as walking. This condition can effect all ages and usually appears in the lower back but sometimes it is present in the neck. Lordosis found in the lower back can give the person an exaggerated posture, which can affect movement and cause pain as well. Some of the factors that can contribute to lordosis include inflammation of intervertebral discs, kyphosis, osteoporosis and obesity. Lordosis is not guaranteed to need medical attention, but when the curve becomes fixed it is advised to see a spinal specialist.
Spondylolysis
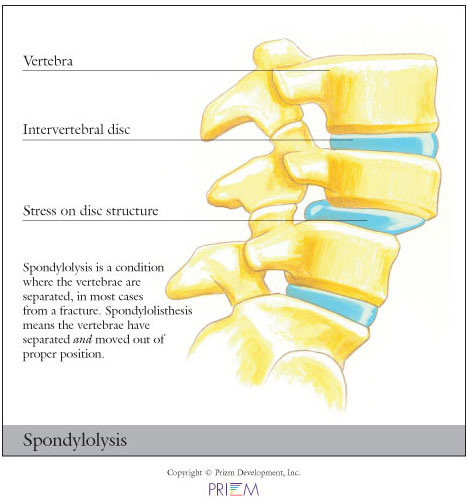 Spondylolysis relates to instability of specific bones in the low back.
It a very common cause of back pain, particularly in adolescents.
Gymnasts who perform routines that bend and arch the back are often
victims of spondylolysis or spondylolisthesis.
Spondylolysis relates to instability of specific bones in the low back.
It a very common cause of back pain, particularly in adolescents.
Gymnasts who perform routines that bend and arch the back are often
victims of spondylolysis or spondylolisthesis.
Causes
Spondylolisthesis and spondylolysis are caused by joint instability
in the low back. The rear part of spinal vertebrae has facet joints
that act as hinges, allowing our spines to twist and bend. Sometimes,
however, the posterior element can crack. Either from heredity or
wear and tear, part of the posterior element called the pars interarticularis
can crack, causing the vertebrae slip forward out of its correct
position. Spondylolysis occurs when the PARS hinge is cracked, but
the vertebrae is still in its correct position. Spondylolisthesis
occurs when the cracked PARS has allowed the vertebrae to slide forward
out of its correct position. If left untreated, spondylolysis can
lead to spondylolisthesis.
[Top]
Craniocervical Scoliosis
Craniocervical problems and Klippel Feil
 We have extensive experience with craniocervical problems in the setting of achondroplasia, Morquio’s Syndrome, other skeletal dysplasias, Ehlers-Danlos, C1 assimilations, congenital basilar invagination, platybasia, and all manner of fractures, instabilities, deformities at the craniocervcial junction.
We have extensive experience with craniocervical problems in the setting of achondroplasia, Morquio’s Syndrome, other skeletal dysplasias, Ehlers-Danlos, C1 assimilations, congenital basilar invagination, platybasia, and all manner of fractures, instabilities, deformities at the craniocervcial junction.
In addition, we also have extensive experience with Klippel Feil syndrome, pediatric cervical stenosis, and other sequelae of congenital abnormalities of the neck in children and adolescents.