Pediatric and Adolescent Scoliosis Surgery
Pediatric and Adolescent scoliosis surgery can be indicated for a wide range of reasons, including unacceptable deformity, pain, paralysis, effect of the curve on sitting or standing, progression of the spinal curve, effect of the curve on lung function, and effect of the curve on aging and degeneration of the low back.
The majority of these pediatric scoliosis surgeries are for idiopathic scoliosis, or genetic scoliosis from anterior spinal overgrowth. Generally, surgery for these curves becomes a good idea around 40-50 degrees in large curves, progress curves, curves that fail bracing, and curves that have a negative effect on the long term health of the paitents.
Currently, the gold standard for these surgeries is single incision, posterior approach, open, high density, 4th generation spinal reconstruction combined with Ponte ostetomies. Research shows that an experienced surgeon (over 10 years experience, scoliosis focused practice) can have a complication rate as low as 2% using 4th generation techniques (Spine Deform. 2019 Jan;7(1):93-99). This effect of surgeon experience is so powerful, that it actually creates better patient reported outcomes (PRO scores), which translates into happier, more functional patients post operatively (Spine Deformity 3 (2015) 496e501).
With these techniques, even large idiopathic curves can have excellent results with excellent curve correction, improvements in appearance, correction of the physical deformity, and return to normal function.
With other types of scoliosis, including congenital (malformed vertebral bodies), neuromuscular (cerebral palsy, spinal bifida) and the syndromes (neurofibromatosis), failed scoliosis surgeries, more complicated techniques might be needed, such as halo-gravity traction, vertebral column resection, hemivertebra resection, pelvic fixation, inter body fusion, and pedicle subtraction osteotomy.
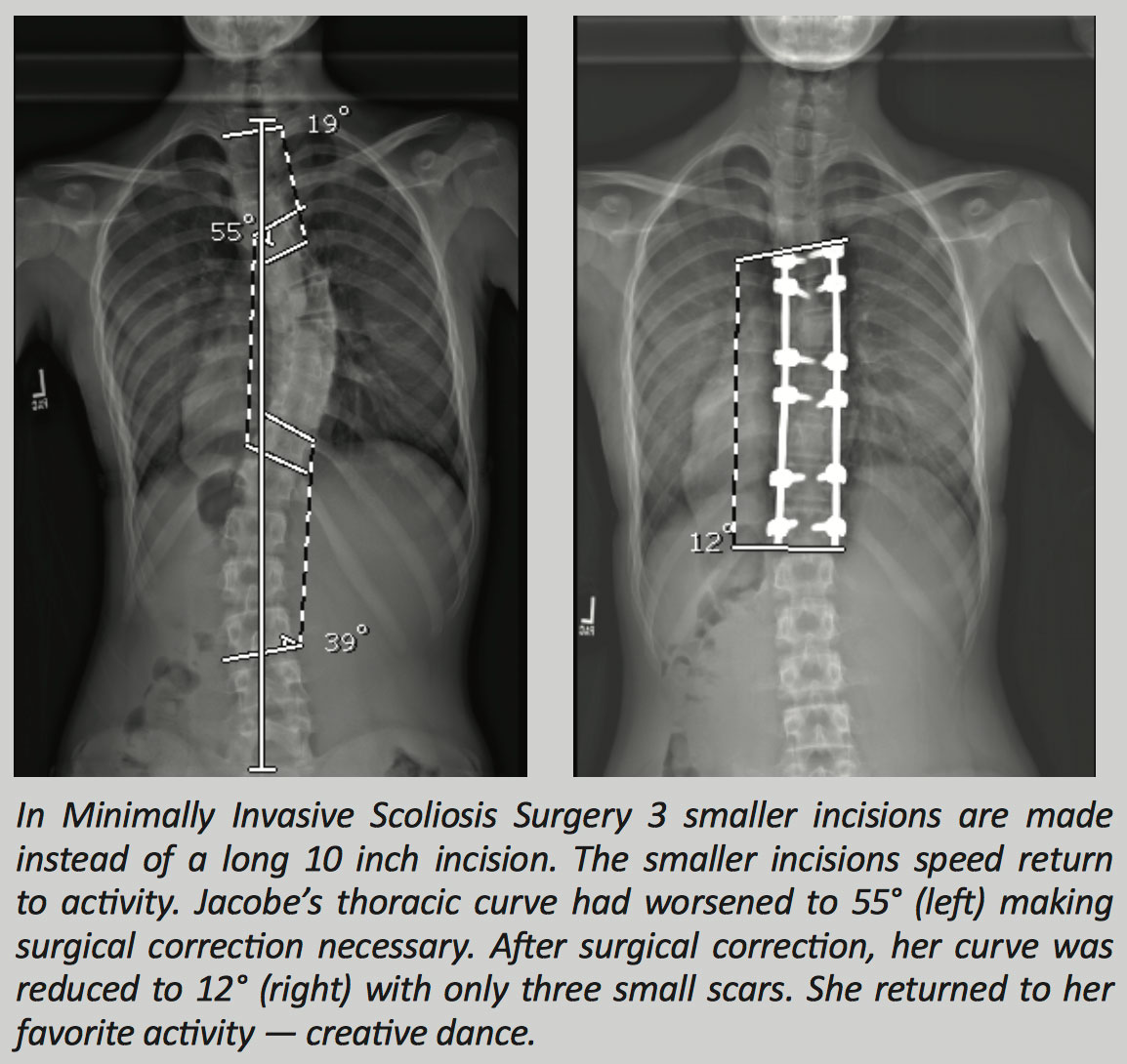 Innovative treatments for pediatric and adolescent scoliosis include minimally invasive scoliosis reconstruction, fusionless scoliosis treatment such as vertebral body tethering or stapling, and less commonly growing constructs in younger patients.
Innovative treatments for pediatric and adolescent scoliosis include minimally invasive scoliosis reconstruction, fusionless scoliosis treatment such as vertebral body tethering or stapling, and less commonly growing constructs in younger patients.
When scoliosis is present before the age of 3, this is known as Infantile Scoliosis. When scoliosis is diagnosed between the ages of 3 to 10, this is known as Juvenile Scoliosis. Children younger than 10 have special needs in scoliosis care.
Whether the cause of the scoliosis is infantile, juvenile idiopathic, congenital, from a connective tissue disorder, neuromuscular, or syndromic, the need for additional spine and rib cage growth to maximize eventual lung function is paramount. Techniques such as growing rods, titanium ribs (VEPTR, vertical expandable titanium rib), or growth modulating procedures (Shilla), are all options to maintain spinal and thoracic growth in young children with spinal deformities. It is important to involve a fellowship-trained spine physician that specializes in spinal disorders, such as scoliosis. Click here to learn more about Dr. Geck at Scoliosis Texas in Austin, he is fellowship-trained in adult and pediatric spine surgery.
Case Study
This 3 year old girl with Ehlers-Danlos syndrome originally presented at the age of 2 with craniocervical instability and quadraparesis. After that was fixed, attention was directed at her early onset severe120 degree scoliosis. Initial set up treatment with growing rods is shown. She was later revised to a more robust growing construct.